August brought more difficult news for the Huntington’s disease community with the halting of yet two more clinical trials. However, Prilenia Therapeutics announced at a major research conference last week that it expects to obtain definitive results from a study of a drug proposed to improve function in the early stages of the disease.
Prilenia CEO and founder Michael Hayden, M.D., Ph.D., a leading HD scientist, reported that the Phase 3 clinical trial of pridopidine is on schedule, with administrators expected to release results early in the second quarter of 2023. (Click here for background on pridopidine, Dr. Hayden, and Prilenia.)
On August 25 Dr. Hayden provided a brief update on the trial, called PROOF-HD (PRidopidine Outcome On Function In Huntington Disease), at HD2022: Milton Wexler Biennial Symposium, sponsored by the HD-focused Hereditary Disease Foundation. It was held August 24-27 at the Royal Sonesta Hotel in Cambridge, MA.
If successful, the PROOF-HD trial will result in a landmark not just for HD, but neurodegenerative diseases in general. Its potential significance has increased because of the disappointing results from two important HD gene silencing clinical trials in March 2021 and the news this month that key trials by Novartis and uniQure had to stop dosing because of safety concerns.
In an August 27 interview with me, Dr. Hayden explained pridopidine’s benefits.
“It's the only drug that has showed some impact on stabilizing TFC [total functional capacity], keeping patients functional, keeping them managing their finances, keeping them at work, keeping them going for walks with their children and grandchildren, keeping them doing activities of daily living for longer,” Dr. Hayden said.
Analysis of pridopidine has demonstrated that patients taking the drug showed a slower decline in TFC. In early patients, pridopidine can maintain TFC and slow deterioration

Dr. Michael Hayden (left) confers with Peter McColgan, M.D., the clinical director for the HD program at Roche, during a break in the Milton Wexler Symposium (photo by Gene Veritas, aka Kenneth P. Serbin)
Neuroprotective effects
The earlier, revised analysis of pridopidine led to a “surprising but very welcome result,” Dr. Hayden continued. Pridopidine works as a “highly potent and highly selective sigma-1 receptor agonist.” An agonist is a drug that mimics a natural substance, while sigma-1 is “a molecular chaperone,” a chemical that helps proteins perform the important function of folding. He called pridopidine “the most potent and selective” sigma-1 agonist ever described.
In everybody’s cells, decreased sigma-1 has a negative impact on monitoring stress, including for the endoplasmic reticulum, a key organelle (subunit) that manages stress. In HD, this subunit experiences disturbances that cause an imbalance in the cell, Dr. Hayden said.
Overall, a reduction in sigma-1 makes neurodegeneration (slow and progressive loss of brain cells) get worse, Dr. Hayden explained.
However, pridopidine enhances sigma-1. The drug has “all in all neuroprotective effects,” by reducing cellular stress and even increasing the critical “connectivity” of the brain and the removal of “toxic products.”
Critically, pridopidine is “the only [HD] drug that has shown stabilization of neurofilament,” an important marker of disease progression, Dr. Hayden observed. An increase in levels of neurofilament, which makes up a brain cell's scaffolding, indicates dysfunction.

A Prilenia poster demonstrating the positive effect of pridopidine on total functional capacity and stabilization of neurofilament (photo by Gene Veritas)
A safe and tolerable drug
PROOF-HD seeks to confirm pridopidine’s efficacy so that it might be approved as a drug by the U.S. Food and Drug Administration (FDA).
“We submitted this to the FDA, and the FDA was hugely supportive,” Dr. Hayden said. Last November the FDA granted pridopidine a “fast track” designation to potentially speed drug approval, because HD is a “significant unmet need,” Dr. Hayden noted.
The designation “allows us to have a closer relationship with the regulators as we go through this process,” he said.
Despite the coronavirus pandemic, PROOF-HD began ahead of schedule in October 2020 and is on schedule to report results in about eight months. It recruited 499 clinical trial volunteers, more than the goal of 480, at several dozen sites in the U.S., Canada, and Europe.
So far, the standard safety monitoring board has found no reason halt the trial.
“So that's also encouraging that this is a very safe and tolerable drug,” said Dr. Hayden.
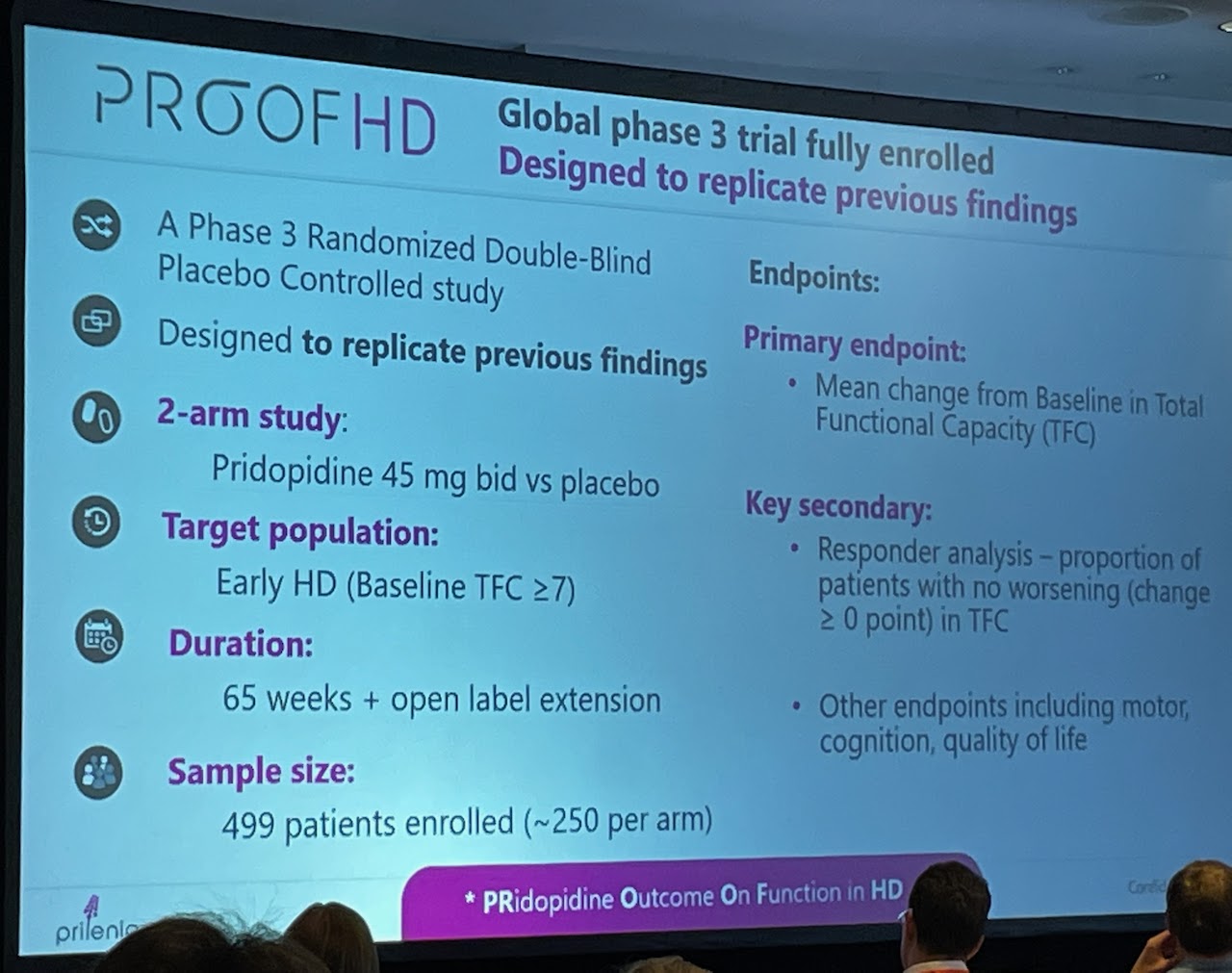
A Prilenia slide with an overview of PROOF-HD, including the main goals (endpoints) (photo by Gene Veritas)
Seeking to prevent disease
In contrast with other top HD drug programs using brain or spinal injections, pridopidine is taken orally twice daily, “without any need for nursing care,” Dr. Hayden pointed out.
If PROOF-HD is highly successful, inviting a priority review by the FDA, Dr. Hayden said that pridopidine could become available for patients in mid-2024.
“My vision for pridopidine is that it could become a standard of care for neuroprotection,” Dr. Hayden stated in a January interview. “For diseases where we can define patients who are close to onset of a neurodegenerative condition, an oral therapy with a benign safety profile – which is what we are trying to establish in our current and planned clinical trials – could become a preventative treatment option.”
In a January 2021 Huntington’s Disease Society of America (HDSA) webinar, Sandra Kostyk, M.D., Ph.D, the co-principal investigator for PROOF-HD in the U.S., referred to pridopidine as a possible “disease-modifying intervention – something that slows the course of the disease.” The data indicate that early-stage HD patients could obtain “long-term beneficial effects” from an approved pridopidine drug for five years or more, she said.
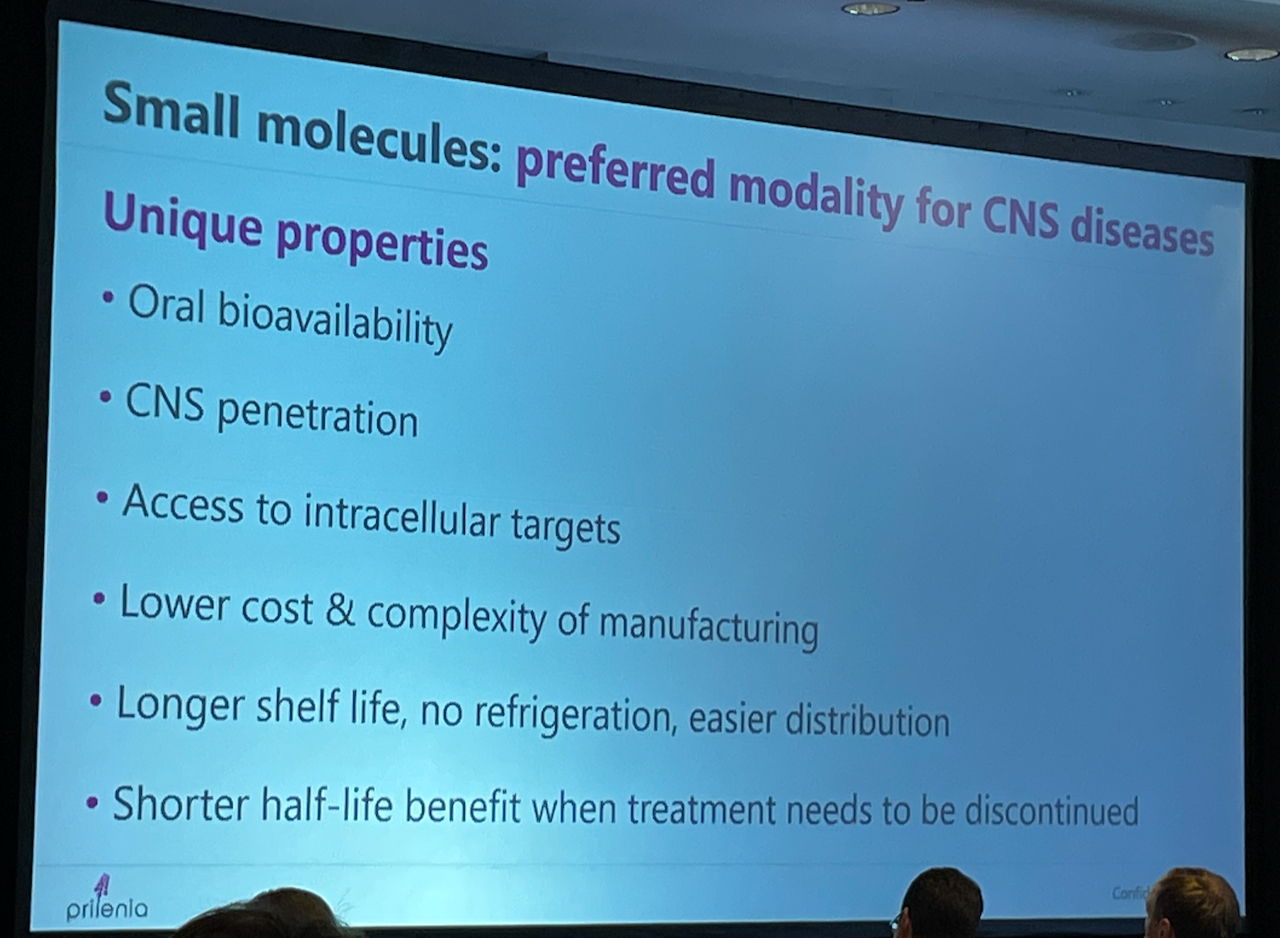
A Prilenia slide about the advantages of small molecule drugs, the preferred method of treatment in HD. Pridopidine is in that category (photo by Gene Veritas)
An upcoming update, a caution, and hope
On September 7, HDSA will host a webinar further updating PROOF-HD and featuring Dr. Hayden, Dr. Kostyk, and Andrew Feigin, M.D., the trial’s principal investigator in the U.S. Click here to register.
“Of course, there's no certainty that this drug will be successful,” Dr. Hayden told me. “Forty percent of Phase 3 trials fail. So, we have a 60 percent chance. In a Phase 3 trial, things fail for all kinds of unexpected reasons, as sadly we've seen in the Huntington's field.”
Pursuing successful trials for pridopidine “has been a long struggle for everybody,” Dr. Hayden concluded. “This is hopeful, but we're not there yet. But hold on as we go on this journey as co-travelers in the attempt to find some way to moderate the course of this dreadful illness.”
(Future articles will cover other aspects of the Milton Wexler Symposium. Also see @HDBuzzFeed on Twitter and this article.)

Dr. Hayden (right) and Nicholas Caron, Ph.D., exchange ideas at the poster session of the Milton Wexler Symposium (photo by Gene Veritas).

